")
")
")
Shoulder Center Saar
Tendon tears in the shoulder
Shoulder tendon tears, also called rotator cuff tears, are common.
Humans require a variety of different tendons for normal shoulder and arm function. As a joint that is almost exclusively controlled by muscles, the shoulder relies on intact tendons. Tendons represent the important link between muscle and bone. Some of these tendons are subjected to significant stress over the course of a lifetime and can therefore wear out and tear.
Often overlooked, tendon injuries lead to pain and increasing functional impairment of the shoulder. If left untreated or treated late, rapid progression of damage can occur, leading to complete loss of function and permanent disability. Unfortunately, many doctors pay too little attention to shoulder tendon injuries, despite significant advances in knowledge regarding functional impairment, prognosis, and treatment in recent years. Unfortunately, even today, there is still far too little differentiation, and all shoulder tendons are often lumped together.
A serious mistake!
Shoulder specialists know that it makes a big difference whether, for example, a long biceps tendon, a Supraspinatus tendon or a subscapularis tendon is damaged.
All of these tendons are located in the shoulder and have their insertions only a few millimeters apart, yet there are huge differences. The prognosis and thus the need for treatment vary fundamentally for each tendon. This is one reason why the diagnosis and treatment of shoulder tendon tears should be left to experienced shoulder specialists. Inappropriate or delayed treatment may be irreversible.
An important function of the tendons in the shoulder is to rotate the humeral head and thus the arm. Because the tendons stretch from back to front around the entire humeral head, they are collectively known as the rotator cuff. However, this should not lead to the assumption that all tendons have the same function and are solely responsible for rotational movement.
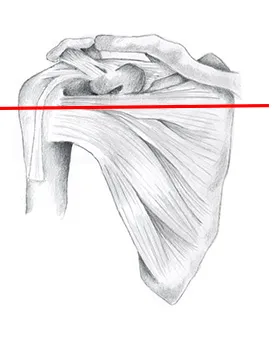
In addition to rotational movements, stabilizing the humeral head is an important function of the rotator cuff. This is illustrated using a few diagrams. The image on the left shows an anatomical drawing of a shoulder joint from the front. Some of the muscles and tendons can be seen as they extend from the shoulder blade to the humeral head.
A section through a shoulder joint at the level of the red line produces the following image when viewed from above.
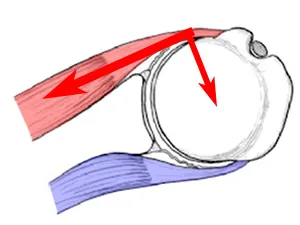
Red marks the Subscapularis muscle with its tendon, and the infraspinatus marked in blue. The subscapularis sits at the front of the shoulder, the infraspinatus at the back of the shoulder blade, and from there, its tendon extends to the humeral head.
The pull of the subscapularis (marked in red) not only causes the arm to rotate inward, but also simultaneously pushes the humeral head backward out of the joint. This results in the humeral head becoming "decentered," and the joint is partially dislocated.
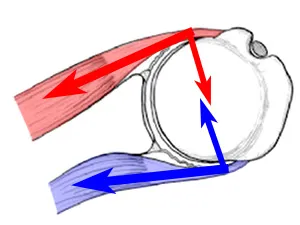
Balance can only be achieved when the infraspinatus muscle, marked in blue and located behind the shoulder blade, contracts in a controlled manner. The infraspinatus prevents the humeral head from slipping backward while still allowing the arm to rotate. This collaboration of several tendons is important for a healthy and, above all, pain-free shoulder. Injuries and tendon tears disrupt this delicate balance.
What pain does a rotator cuff tear cause?
When the rotator cuff is damaged, those affected often complain of stabbing pain, especially with any upward or backward movement of the arm. The arm's strength when lifting is often reduced. The inflammation of the bursa that usually develops also frequently leads to nighttime shoulder pain, which regularly radiates into the upper arm. Some patients even describe pain radiating into the hand.
How can we diagnose a tendon tear?
When describing the circumstances of the accident or the exact symptoms, the specialist will suspect a rotator cuff tear. Special tests during the examination, These specifically target the individual muscles and tendons of the rotator cuff, providing information about functional limitations or loss. Pressure on the tendon attachments and specific pain points completes the examination.
Enormous advances have also been made in the field of imaging in recent years. Improvements in ultrasound technology now allow most tendon tears to be detected quickly and reliably. Unfortunately, even these devices still vary enormously in quality, which is easily reflected in the purchase price. Really good ultrasound devices with correspondingly high image resolution, digital image processing, and 3D scanning still cost as much as a sports car and are usually only available in specialized centers. We are pleased to be able to offer our patients such a sophisticated device for shoulder diagnostics.

One advantage of ultrasound over magnetic resonance imaging is the possibility of dynamic examination, meaning the shoulder can be moved during the examination. This allows the tendon to be examined even under load.

Magnetic resonance imaging can also depict tendon tears. In addition to the location and size of the defect, MRI can also provide information about degeneration of the associated muscle. This muscle atrophy in tendon tears, often referred to as fatty degeneration, must be assessed. It provides information about the prognosis for any surgical treatment. However, even conventional MRI is not always able to reliably depict tendon tears. The procedure can be enhanced with MRI arthrography. Here, a contrast agent is injected directly into the patient's shoulder before the examination. This allows even smaller defects that would otherwise remain hidden to be visualized.
When is a rotator cuff tear treated?
A torn tendon doesn't heal on its own. However, not every tendon tear needs to be or can be closed surgically. The specialist must decide whether the patient can live with a torn tendon and be symptom-free in the long term, or whether the damage to the shoulder joint requires repair.
Until a few years ago (around 2010), this decision was based solely on the patient's age. For example, younger patients would undergo surgery, while older patients would undergo physical therapy. Unfortunately, many doctors still reduce their treatment decisions to this simple formula.
The results show that considering only age often leads to catastrophe for the patient.
Today, in addition to age, specific living conditions, and personal functional requirements, the individual pathology (type of tendon tear) must be taken into account. Above all, the precise differentiation of the affected tendon, the type and size of the tear, degeneration of the tendon and muscle, and the assessment of associated damage are crucial in making a treatment decision. However, this requires considerable experience and expertise to make this decision. Apart from specialists in this field, most other physicians are often overwhelmed by the decision.
You must have the Adobe Flash Player installed to view this player.
What is the treatment for a rotator cuff tear?
Tears up to a certain size can be repaired through arthroscopic surgery. While years ago this was only possible for very small tears, if at all, new instruments now allow even larger tears to be repaired minimally invasively. For reconstruction, the torn tendon ends are sutured to the bone using tiny implants made of titanium, plastic, or bioresorbable materials. Pictured at left is a Healicoil suture anchor.
This modern screw consists almost entirely of a plastic thread with internal threads. The original screw has a diameter of only 4.5 mm.
However, not every tendon tear requires surgery. In the case of a very large tear, perhaps one that has been present for several years, attempting surgical reconstruction may even result in worse results than without surgery. In this case, the physician must decide for each patient individually whether surgery is necessary or whether conservative treatment might be a better option. Even conservative treatment—i.e., treatment without surgery—leads many patients to freedom from symptoms and good strength and mobility of the shoulder.
The mainstay of conservative treatment is targeted exercises and training to restore shoulder function. It's important to build up the muscles that compensate for the loss of the torn tendon. At the same time, efforts must be made to optimally stabilize the humeral head in its socket. Our shoulder guide contains a collection of various exercises that can be used for this purpose.
If this conservative therapy does not lead to the desired success, a small arthroscopic operation can be performed to smooth the torn tendon stumps and remove inflamed tissue, such as a chronically inflamed bursa.