")
")
")
Shoulder Center Saar
SLAP – lesion
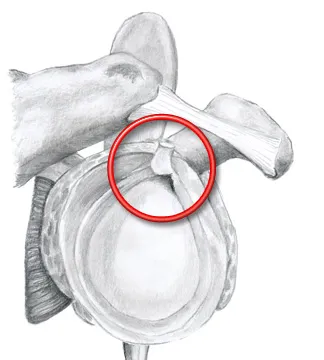
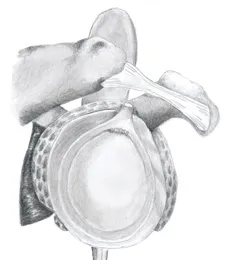
Because the bony socket of the shoulder is very small compared to the humeral head, the shoulder joint is insufficiently stabilized by bone. To prevent dislocation of the shoulder joint, a joint lip, also called the labrum, surrounds the entire bony socket. This joint lip considerably enlarges the socket and, thanks to its flexibility, still allows the humeral head a high degree of range of motion.
The tendon of the long biceps muscle is attached to the upper extension of this labrum. The area of the upper labrum and the insertion of the long biceps tendon is also known as the labrum-biceps tendon complex.
Damage to the labrum-biceps tendon complex is referred to as a SLAP lesion. SLAP is an Anglo-American acronym for "Superior Labrum Anterior to Posterior."
The injury can be caused by various accidents or excessive strain. This can include a sudden and unexpected pull or pressure on the already tense biceps tendon. This could be a fall on an outstretched arm, in which the humeral head kicks upwards, shearing off the tendon insertion and the articular lip, or a sudden lifting of a heavy load, in which the long biceps tendon is so tensed that it tears off the bone along with the articular lip.
Another common cause is considered to be microtraumatic damage to this area. Frequent extreme throwing movements, such as those encountered in baseball, handball, or javelin throwing, result in extreme abduction and external rotation of the humeral head. This leads to torsional stress at the origin of the long biceps tendon. As the throwing movement continues, the torsional forces can cause the upper joint lip to peel and lead to fiber tears. The repeated stresses then gradually lead to the damage spreading.

How is the diagnosis made?
Techniques such as ultrasound and magnetic resonance imaging are not always possible with certainty. Only by considering many individual components can the suspicion of a SLAP lesion be confirmed.
Diagnosis of SLAP lesions includes a comprehensive clinical examination, as well as a medical history. The medical history can provide extensive information about the mechanism of the injury, the development of pain, any existing feeling of instability, and the type and level of sport practiced.
Numerous special tests are available for diagnosing a SLAP lesion during clinical examination. Since even a standard MRI scan often does not provide the desired diagnostic certainty, many specialists recommend a special contrast agent study. This involves injecting a special contrast agent into the shoulder joint prior to the MRI scan. The subsequent examination allows for a much better assessment of the tendon insertion and labrum. However, this examination cannot determine the exact type of lesion. This can only be reliably identified with the help of arthroscopy (arthroscopy).
Einteilung der SLAP Läsionen:
SLAP lesions are classified according to the type of damage and are divided into four groups according to Snyder. Type II is usually further subdivided into three subtypes a-c, which allow for a more detailed description of the damage.
-
Type II a:
Tear of the long biceps tendon and the adjacent anterior labrum from the superior glenoid (shoulder joint socket). The injury affects the biceps anchor (attachment point of the biceps tendon) and the anterior-superior labrum.
-
Type I:
Degenerative changes of the superior labrum and biceps insertion without detachment but fraying.
-
Type II b:
Tear of the long biceps tendon and the adjacent posterior labrum from the superior glenoid rim (shoulder joint socket).
The damage affects the biceps anchor (attachment point of the biceps tendon) and the posterior-superior labrum.
-
Type II c:
Tear of the long biceps tendon and the adjacent anterior and posterior labrum from the upper glenoid rim (shoulder joint socket rim).
The damage affects the biceps anchor (attachment point of the biceps tendon) and the labrum front and back above.
-
Type III:
Basket-handle lesion of the superior labrum with intact biceps tendon insertion
-
Type IV:
Longitudinal alignment of the long biceps tendon with dislocation of a labrum-biceps portion downwards into the joint space
Die Therapie der SLAP-Läsionen
Treatment of SLAP lesions requires a differentiated approach depending on the type of lesion. Types I and III SLAP lesions are generally debrided, meaning loose tissue is removed so that nothing can become trapped in the shoulder. Types II and IV lesions are treated with suture anchor techniques, meaning the torn-off portions are reattached arthroscopically.
You must have the Adobe Flash Player installed to view this player. The Grade 4 SLAP Lesion according to Habermayer The above video shows the shoulder of a young patient who sustained a complex 4° SLAP lesion after a shoulder dislocation. Furthermore, an anterior and posterior labral detachment (Bankart lesion) was found.