")
")
")
Shoulder Center Saar
AC joint injury
In a shoulder joint dislocation, the capsule and ligaments of the acromioclavicular joint, the joint between the collarbone and shoulder blade, tear.
Acromioclavicular joint injuries typically result from a direct fall onto the shoulder. The most common cause is a sports-related accident. This injury is very common in mountain biking, motocross, skiing and snowboarding, martial arts, and soccer goalkeepers.
The acromioclavicular joint, also called the acromioclavicular joint, is the connection between the outer end of the collarbone (clavicle) and the acromion of the shoulder blade. The acromioclavicular joint is stabilized by a tight joint capsule and several ligaments. In a shoulder joint dislocation, the capsule and ligaments of the acromioclavicular joint are strained or can even tear completely.
The symptoms of acromioclavicular joint injury
After a fall on the shoulder, the affected person with a shoulder joint dislocation immediately experiences pain in the shoulder, particularly above the acromioclavicular joint. This pain intensifies when the arm is moved. Therefore, the arm is usually held in a typical protective position close to the body. In a shoulder joint dislocation with a tear in the supporting ligaments at the joint, the outer end of the collarbone typically becomes elevated.

How does the doctor diagnose acromioclavicular joint dislocation
The diagnosis of a shoulder joint dislocation can often be made based on a physical examination and thorough questioning. Usually, swelling and precisely localized tenderness are found over the acromioclavicular joint.
If the ligaments are partially or completely torn, the outer collarbone is misaligned, causing the skin in this area of the shoulder to bulge upward.
The upwardly displaced collarbone can be moved downward by applying pressure. Doctors refer to this phenomenon as the piano key phenomenon.
To ensure a reliable diagnosis and rule out further injuries, an X-ray of the shoulder joint is also required. If the findings are unclear, functional images of both joints can be taken, comparing them side by side. The patient holds a heavy weight in each hand while standing. Both shoulder joints are then X-rayed. By comparing the position of the raised clavicle, the severity of the injury can be assessed.
Shoulder dislocations are classified according to their severity. Currently, the most common classifications are the Tossy classification and the somewhat newer Rockwood classification.
The classification according to Tossy and Rockwood
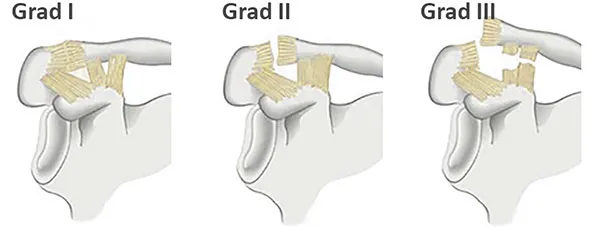
The Tossy classification has 3 grades and the Rockwood classification 6 grades, with the first three grades being identical in both classifications
- Grade I: The ligaments are torn without the joint parts shifting against each other.
- Grade II: The ligaments of the joint capsule are partially torn and the joint parts are slightly displaced.
- Grade III: All ligaments of the acromioclavicular joint are torn. The outer end of the clavicle protrudes approximately the width of the shaft (1-1.5 cm) upwards.
The therapy
Depending on the severity, the injured shoulder is treated differently. Tossy I and II injuries (Rockwood I and II) with strains or partial tears of the ligaments are treated conservatively, i.e., without surgery. The shoulder joint is temporarily immobilized and the joint is cooled. If the clavicle is slightly elevated, a special bandage or brace can be applied to relieve pressure on the joint. Physiotherapy follows.
Things get complicated with a Tossy III injury. Because not all Tossy III injuries are the same, the decision between conservative or surgical treatment must be abandoned based on the Tossy classification and the more precise Rockwood classification must be used.
In the past, Rockwood III injuries involving complete rupture and tearing of the ligaments were always treated surgically. However, recent studies show that surgery does not always produce satisfactory results. In fact, when analyzing symptoms, function, and patient satisfaction, almost all studies found no difference between surgically treated and conservatively treated patients.
The Rockwood IV injury describes a special case in which horizontal instability in the acromioclavicular joint is the primary cause. The shoulder blade tilts forward. This injury can also be treated conservatively. The goal of treatment is muscular stabilization of the shoulder blade. This prevents the shoulder blade from tilting forward.

Treatment for a complete Rockwood V shoulder joint dislocation with completely torn ligaments is usually surgical. Only through surgery can the correct anatomy of the joint be restored. Since these patients not only have torn capsules and ligaments, but also the deltotrapezoid fascia, significant instability occurs. The shoulder and shoulder blade tilt sharply forward, and the clavicle protrudes significantly. This effect can usually be significantly amplified by applying traction to the arm. In these cases, surgical treatment is often more promising than conservative therapy.
During shoulder dislocation surgery, the torn ligaments are sutured and the shoulder joint temporarily splinted. The difference between the various surgical methods lies in the splinting. It can be performed with screws, plates, wires, or even special suture systems. Each system has its advantages and disadvantages. Since wires often break, they are rarely used today. Among the plating systems, the so-called hook plate has become established. Here, a plate is screwed onto the outer end of the clavicle. The plate has a hook with which it "hooks" under the acromion, preventing the outer end of the clavicle from rising. The major disadvantage of this procedure is that the patient cannot raise their arm above the horizontal for 3-4 months, and the plate must be surgically removed.
Specialized suture systems have also become established as an alternative to the hook plate. The operation is certainly somewhat more difficult than inserting a hook plate, but in the hands of an experienced surgeon, the results are excellent. In this procedure, a hole is drilled from the top of the clavicle to the underlying bony protrusion of the shoulder blade using a targeting instrument. A kind of pulley mechanism made of sutures is then pulled through. The sutures are held in place at the top and bottom by small metal studs. At the end of the operation, only these metal studs are visible on the X-ray image.

The major advantage of this procedure is that it can be performed arthroscopically, eliminating the need to cut open the shoulder. Furthermore, metal removal isn't necessary.
For a period of six weeks, until the ligaments and capsule heal, the joint is usually immobilized with a shoulder immobilizer. After that, the joint is gradually mobilized, and the muscles are strengthened with physiotherapy. If a hook plate has been inserted, it often has to be removed in a second operation after 3-4 months.
Can I do sports again?
A shoulder joint injury is a relatively benign injury. After healing, more than 90 percent of those affected experience no discomfort in everyday life or during sports. However, in a small proportion of those affected, particularly after Grade II and Grade III injuries, pain or chronic joint instability may persist. The arm's function is then limited. A rare late consequence of a shoulder joint dislocation is premature wear of the joint, acromioclavicular joint arthrosis.